
The Situation
Banji, you told me where you are. Client acquisition has slowed, and it's your focus right now. You've got people who aren't optimized, not enough new business coming in to keep them busy. Your marketing team can create nice designs, but they've been stuck on the technical side, and the Google Ads haven't been bringing in the right leads.
So you looked at a done-for-you agency. They run the Meta and Google ads and an AI follow-up system, and they guarantee a revenue number. Test them, by all means. If they hit the leads they promise, that's a good deal, and you should find out.
But you already put your finger on the catch:
"They run the ads, I don't own the, you know, they own everything." Banji
The ads, the CRM, the automation, the leads, all of it lives on their side. That's fine for a few months of learning what works. The real question isn't whether you need more leads. You do. It's the long game.
Do you rent that growth engine forever, one line at a time, or use this moment to build and own the same machine while you learn from them?
What This Is Really Costing You
The visible cost you feel already: the slow pipeline, a marketing team that can create but can't crack the technical side, and capacity you're paying for with not enough business to keep it busy. The cost that's easy to miss is a cost of ownership, not cash flow.
The per-line rent, if it becomes permanent
The agency charges per service line, roughly $16,000 to $20,000 a cycle. One test run is one thing. But you already told me where you want to take this:
"I can replicate that with VA. I can replicate that with Medicaid. I can decide to do private pay." Banji
Run all three their way, indefinitely, and it's six figures a year, forever, for infrastructure that's never yours.
You never own the asset
Every dollar of ad spend you put through their system makes their asset better, not yours. You can't see under the hood, improve it, repackage it, or resell it. Which is exactly where your head already is:
"If you can figure out a way to package these automations and things like that, that's what they figured out." Banji
They figured out how to own a machine and rent it to home-care agencies like yours, 75 of them since April, by your own count. That's the side of the table you want to be on.
What I Heard You Want
Here's what I took from our call. Flag anything that's off.
- Own the infrastructure outright, in your name. Not a login to someone else's account.
- Run it side by side with the agency. Let them prove VA while you build and own Medicaid, then compare.
- Replicate across lines. Build once, point it at VA, then Medicaid, then private pay.
- Package and resell it eventually, instead of renting the kind of asset they built.
- Speed and qualification without a human on the phone. Instant first contact, then an AI that only hands your team the leads worth their time.
Where the Real Work Is
You know this isn't a weekend automation. Here's where the real work sits, and what your money is actually buying.
You asked me to design the funnel structure, not just spin up an account, and that's the right call. The pipeline (how a lead moves from new, to qualified, to nurture, to disqualified, and what fires at each step) is the spine of the whole system. Designed once, built to flex as you add VA, Medicaid, and private pay, it's the part you own and reuse across every line.
The moment your AI asks "are you on Medicaid?" or a caller says "my mom has dementia," that conversation becomes protected health information, and every tool that touches it needs a signed agreement. The Meta form stays clean, no health questions, because Meta won't sign a BAA. The CRM, voice agent and AI brain all sit inside compliant infrastructure. It's not clear the agency is even handling this. It's the exact ground your two live systems already run on.
An AI that sounds robotic or breaks character loses a stressed family in the first thirty seconds. Making the voice and SMS agents sound genuinely good, empathetic and on-brand, is its own craft. They have to hold up when a caller says "my mom has dementia, I don't know what Medicaid is," stay in character, pull the four things that qualify a lead (location, timeline, funding, decision-maker), route it without inventing an answer, and run both channels without bombarding the lead with the same questions twice.
The whole point is that it's yours, and that changes how it's built. Accounts in your name, documented and labeled, so you can improve it, extend it to the next line, and one day resell it. A design decision made up front, not a vendor black box.
The System
From the moment a lead lands, through qualification, to the alert on your team's phone. Everything right of "New Meta Lead" runs on infrastructure you own.
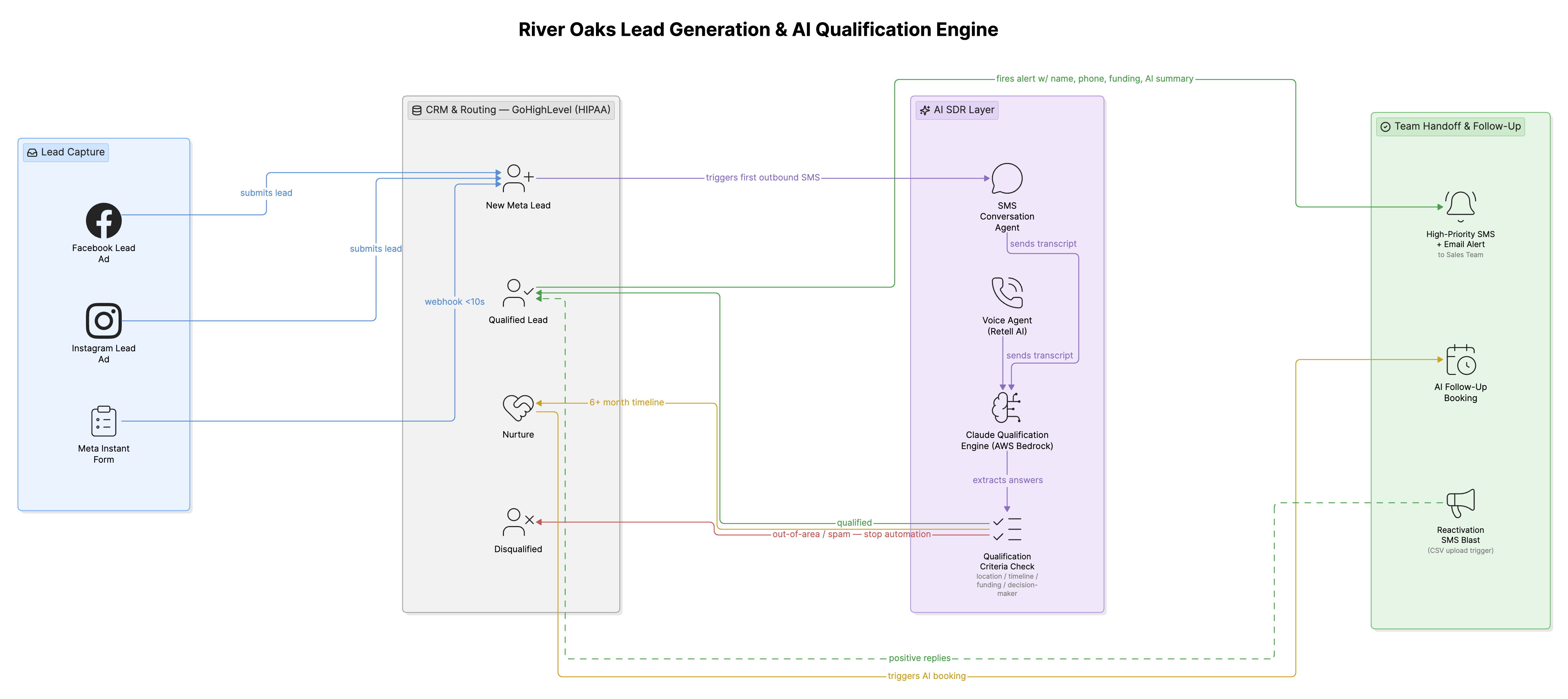
Meta captures the lead. GoHighLevel routes it. The AI layer qualifies it. Your team only touches the leads worth touching. (Click to open full size.)
What you get
- A GoHighLevel sales pipeline designed and built in your name: the funnel structure (New Meta Lead, Qualified, Nurture, Disqualified), HIPAA-enabled, documented, and structured to flex as you add lines.
- Instant first contact: Meta Instant Form to CRM, first message out in seconds, because fast response is what actually closes.
- AI qualification on SMS and voice against your four criteria, empathetic and on-brand, with channel logic that doesn't bombard the lead.
- Three-way routing: qualified leads fire an instant SMS and email to your team (name, phone, funding, summary); not-right-now goes to Nurture; out-of-area and spam get disqualified.
- Reactivation: upload a CSV of cold past leads and the AI re-engages by SMS, routing positive replies back to you.
- Full HIPAA compliance and a documented handoff, so it's an asset you can extend to the next line.
- Not in scope: the Meta and Google ad campaigns and creative. Your marketing team and the agency handle the ads; this is the engine behind them.
Timeline & What I Need From You
Four to five weeks from the kickoff call, not from the date you sign. Week one is kickoff, account and compliance setup (GoHighLevel HIPAA activation and signed agreements), and gathering your inputs, in parallel with the build. From there it's the qualification engine, routing, alerts and reactivation workflow, then testing on real conditions and go-live on your first line (we discussed Medicaid). The pace is tied to how fast access and inputs come back to me.
What I need from you
- GoHighLevel account created in River Oaks' name. I build inside it, you own it.
- Signed HIPAA agreements with the stack, and Meta / Facebook ad account access for the lead-form connection.
- The agency's VA and Medicaid ad examples, to reverse-engineer the qualification and messaging.
- Knowledge-base content: services, funding and eligibility (VA, Medicaid, private pay), service area, common questions.
- Team contacts for the alert, the calendar Nurture books into, and your reactivation list (with confirmation those contacts agreed to be texted, which stays your side).
You'll get a weekly update and a same-day response through the build. You'll never wonder where things stand.
Investment
Two ways to do this, same build in both. The difference is whether you add a month of hands-on support once real leads start hitting the system. Either way, the first payment is the same $3,450. Pick one below.
- The complete HIPAA-compliant lead engine, on your accounts, live on your first line
- One round of revisions on the core system
- 30-day warranty
- Everything in Option A
- A month of hands-on support once real leads hit it: up to three rounds of revisions, agent tuning on real transcripts, qualification adjustments, a team training call with a recording and one-page SOP, plus priority turnaround
- 30-day warranty
The same $3,450 gets the build going either way. Option A's second payment is due on confirmed delivery. Option B keeps that and adds a final $1,500 at the end of the support month, once you've watched it run on real leads. Both come with a 30-day warranty: if something isn't doing its core job, I fix it.
Platform costs go to the providers, not me. GoHighLevel's HIPAA plan is about $297 a month; voice, messaging and AI usage are usage-based and modest. They're yours, and part of what owning it means.
The bottom line
The agency path is $16,000 to $20,000 per line, recurring, for an asset that stays theirs. This is $6,900 once, plus about $300 a month you'd pay on any version of this, and you point it at VA, then Medicaid, then private pay at no extra build cost per line. It doesn't take many new private-pay clients to cover that, and set against the agency's recurring rent it pays for itself early and then keeps paying.
Why Me, and What Happens Next
You already know how I work. Two of your systems run on your infrastructure right now, the EVV timesheet automation and the EOP-to-QuickBooks reconciliation, both HIPAA-grade, both yours, saving you more than $48,000 a year between them. This isn't a first date. The agency rents you leads and keeps the infrastructure. I build you the asset, in your name, documented, ready to scale to the next line, the way I came up building for a $35M-plus D2C portfolio: like an owner would. Which is what you're becoming.
Next steps
You're already testing the agency on VA. The smart move is to build and own the Medicaid line in parallel, and see for yourself which one you'd rather have your name on. Let's get the kickoff booked this week.
Systems We Can Build Next
You raised most of these yourself, so they're on the record: a caregiver compliance dashboard (replace the license and TB-test spreadsheet with a live view of what's missing, which you flagged as quick and high-value), an AI ad-creative agent that generates video ads once your strategy is dialed, and a client portal you could productize and resell. None are scoped or priced here.